Anti-Müllerian hormone levels (AMH) are an important marker for ovarian reserve and egg quality. These levels vary during the natural menstrual cycle as well as during ovarian stimulation for IVF-ICSI treatments. Discovered in the 1980s as a hormone synthesized by the ovary, AMH regulates the different stages of folliculogenesis and has neuroendocrine effects. Serum AMH has emerged in the past few years as one of the most reliable and important markers of ovarian reserve in assisted reproductive technologies (ART).
Ovarian reserve represents the absolute number and functional capacity of follicles and germ cells, which can affect a patient's response to ovarian stimulation as well as their chances of success with ART. Assessing ovarian reserve to predict oocyte retrieval marks a major challenge in ART — AMH and antral follicle count (AFC) may be the most reliable predictors of ovarian reserve.
What Is the Best Time To Measure Anti-Müllerian Hormone Levels?
AMH is thought to be a reliable marker of ovarian reserve that gives an accurate measurement regardless of the cycle phase. However, recent research from Pulsus found that during ovarian stimulation, the Anti-Müllerian hormone test shows both inter- and intra-cycle variations that cannot be explained purely by analytical variability.
In a patient's natural menstrual cycle, serum AMH levels are higher in the follicular phase compared with the luteal phase regardless of their ovarian reserve levels. Younger patients typically have a distinct pattern of intra-cycle fluctuation, and short-term inter-cycle variations have also been reported.
With such fluctuation, when is the best time to measure AMH? The initial 1–3 days of the menstrual cycle before beginning ovarian stimulation may offer the most consistent results overall.
How Does an Antral Follicle Count Complement an AMH Test?
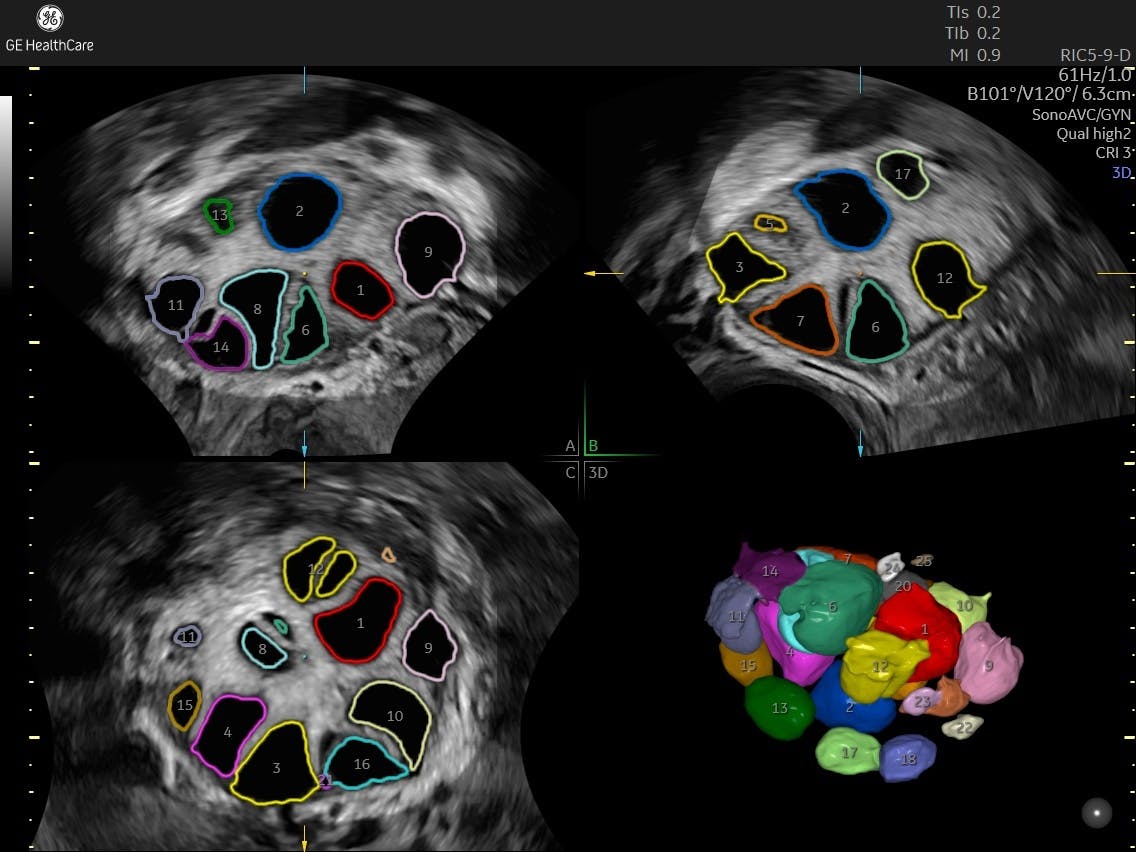
When measured via ultrasound such as three-dimensional SonoAVC™️, antral follicle count (AFC) has been found in a study from Reproductive Biology and Endocrinology to correlate closely with conventional 2D transvaginal ultrasound and serum levels of Anti-Müllerian hormone in patients with infertility. 3D ultrasound, however, was shown to yield a more accurate result than when using 2D technology. 3D ultrasound also carries visual advantages when there are more than 20 follicles to count, and it requires less time for examination.
Due to the variability of AMH levels, thorough evaluations can be made by including not only AMH levels but also AFC measured with ultrasound during the early follicular phase. This provides more accurate information about ovarian reserve and the prognosis for ovarian stimulation. It can also be used to determine the ideal dosage of medication. Although AMH alone is an important biomarker for ovarian reserve, correlating AMH levels with AFC count can help clinicians deliver an accurate assessment of ovarian reserve and egg quality during IVF-ICSI treatment.